
.jpg)
Oral Pathology
 photo")
Andrew Bigelow (he/him/his)
Dental Student
Children's Hospital Colorado, Aurora, CO
University of Colorado School of Dental Medicine
Denver, Colorado, United States
Catherine M. Flaitz, DDS, MS
Professor and Chair, Diagnostic Sciences; Adjunct Pediatric Dental Faculty
University of Colorado School of Dental Medicine, Aurora, CO
Aurora, Colorado, United States

Shahbaz Katebzadeh, M.S., D.M.D
Resident
Children's Hospital Colorado
Aurora, Colorado, United States
 photo")
Chaitanya P. Puranik, B.D.S., M.S., M.Dent.Sci., Ph. D. F.A.A.P.D., Diplomate (he/him/his)
Residency Program Director
Children's Hospital Colorado
Children's Hospital Colorado and School of Dental Medicine, University of Colorado Anschutz Medical Campus
Aurora, Colorado, United States
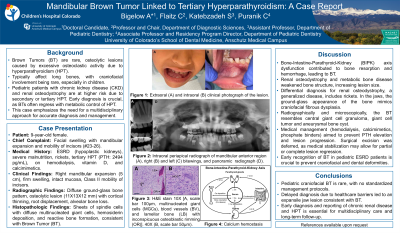
Introduction: Brown tumors (BT) are rare, non-neoplastic, osteolytic lesions associated with hyperparathyroidism (HPT). BTs are rare in the craniofacial region.
Case report: A nine-year-old female presented with significant cortical expansion of the anterior, right mandible with an intact mucosal surface and mobility of teeth (#s24-26). Medical history included end-stage renal disease secondary to hypoplastic kidneys, severe malnutrition, and tertiary HPT (2494pg/mL). Blood urea nitrogen (68mg/dL), calcium (12.3mg/dL), creatinine (4.1mg/dL) values were elevated. Panoramic radiograph revealed diffuse, ground-glass appearance of bone, consistent with renal osteodystrophy. CT imaging exhibited a well-circumscribed, osteolytic lesion of the mandibular, right, parasymphyseal region (11X13X12cm) with cortical thinning. Histopathologic examination demonstrated a giant cell lesion, consistent with BT. Patient received regular hemodialysis along with vitamin D supplements and calcimimetics.
Conclusion: Management of BT ranges from conservative intralesional steroid injection to recontouring/excision. Control of chronic renal insufficiency and HPT can lead to partial or complete resolution of BT.
Identify Supporting Agency and Grant Number: Not applicable