
.jpg)
Syndromes/Craniofacial Anomalies
 photo")
Jenna M. Panek, DMD (she/her/hers)
Resident
Cincinnati Children’s Medical Center Hospital, Cincinnati, OH
Cincinnati Children's Hospital Medical Center
Cincinnati, Ohio, United States
Elizabeth Gosnell, DMD
Cincinnati Children's Hospital Medical Center
Jeffrey Lee, DDS
Cincinnati Children's Hospital Medical Center
Jue Wang, DDS, PhD
Orthodontist/Assistant Professor
Cincinnati Children's Hospital Medical Center
Cincinnati, Ohio, United States
Jue Wang, DDS, PhD
Orthodontist/Assistant Professor
Cincinnati Children's Hospital Medical Center
Cincinnati, Ohio, United States

Scott Schwartz, DDS, MPH
Associate Professor
Cincinnati Children's Hospital Medical Center
Cincinnati Children's Hospital Medical Center
Cincinnati, Ohio, United States
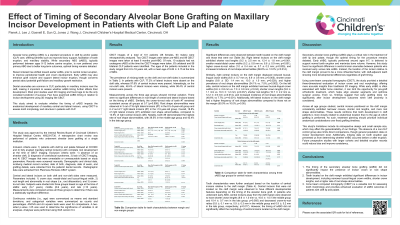
Purpose: Secondary alveolar bone grafting (sABG) is typically performed between 9 and 12 in patients with cleft lip and palate, prior to canine eruption. Recent studies propose a shift toward synchronizing sABG with eruption of maxillary central incisors to prevent compromised development. However, there is lack of evidence showing that late sABG leads to more incisor abnormality. We aimed to explore the impact of the timing of secondary alveolar bone grafting on maxillary incisor development.
Methods: Parameters including crown size, root length, and crown-to-root ratio were measured on cone beam computed tomographic (CBCT) images for central and lateral incisors. Data was divided into three groups based on the age of which sABG was performed: early (6-7 years old), middle (8-9 years), and late ( >10 years old).
Results: CBCT images of a total of 101 patients (38 females, 63 males) were retrospectively analyzed. No significant differences were found in crown size and root length/shape of central and lateral incisors depending on the time at which sABG was performed. However, differences were observed in teeth on the margin of the cleft versus teeth that were not on the cleft margin. Central incisors on the cleft margin were observed to have smaller buccal-lingual crown widths, shorter crown lengths, and a higher rate of root shape abnormalities when compared tothose that were not on the margin.
Conclusions: Patients who receive late secondary ABG did not show a higher rate of maxillary central incisor anomalies when compared to patients who receive early secondary ABG.